Ref. No:IRDA/RI/GDL/MISC/015/01/2021
Date:22-01-2021
Guidelines on Cross Border Re-insurers
In exercise of the powers conferred under Sec. 34 (1) of the Insurance Act, 1938 read with Reg. 4 (3) of the IRDAI (Re-insurance) Regulations, 2018, the Authority hereby makes the following Guidelines.
These Guidelines aim to streamline the regulatory process with respect to cross border reinsurers and will supersede existing Guidelines No. IRDAI/NL/GDL/RIN/017/ 01/2016 dated 19th January, 2016, on CBRs.
1. Allotment of Filing Reference Number (FRN) to CBRs:
a. All Cross Border Reinsurers (CBR) shall necessarily comply with the eligibility criteria as stipulated in Reg. 4 (1) of the IRDAI (Re-insurance) Regulations, 2018.
b. Filing of application for allotment of FRN to CBR shall be commensurate with Re-insurance programme of the insurer, as submitted with the Authority in terms of the IRDAI (Re-Insurance) Regulations, 2018;
c. The insurer who wish to place re-insurance business with CBR shall file an online application with the Authority in the form as specified at Annexure – 1, for allotment of FRN for CBRs under the category of Eligible CBR or Non-Eligible CBR, as the case may be;
d. The Authority may raise any other requirements if necessary for processing of such application for allotment of FRN to CBR. After examination of submissions made by the insurer the Authority may allot system generated FRN to the CBR within three (3) working days from receipt of last document;
e. All the re-insurance business placements made with the Cross border reinsurers who do not comply with Eligibility Criteria, shall be placed before the Board of Directors of the insurer for their approval / ratification, and certified copy of such resolution shall be filed with the Authority;
2. General Provisions:
a. The insurer shall not transact re-insurance business with any CBR without valid FRN;
b. The Authority will allot country wise separate FRN to the CBR;
c. The FRN allotted shall be valid for one financial year for which application is filed by the insurer;
d. Once FRN is allotted for any particular CBR the same may be used by other insurer for placement of re-insurance business with such CBR;
e. The insurer, within thirty (30) days of the commencement of the financial year, shall submit a certificate of compliance (in Annexure-2) to the Authority confirming that, the re-insurance placements made to CBRs who comply with the eligibility criteria or with those CBRs prescribed in these guidelines. This certificate is to be filed with the Authority along with submissions required to be made under Reg. 3 (3) (A) (c) of the IRDAI (Re-insurance) Regulations, 2018;
f. Notwithstanding anything contained in these guidelines, the insurer shall comply with the Insurance Act, 1938 and other applicable regulations issued by the Authority from time to time.
These Guidelines shall come into force from the date of notification.
Suresh Mathur
(Executive Director)
INSURANCE REGULATORY AND DEVELOPMENT AUTHORITY OF INDIA
INSTRUCTIONS FOR FILING APPLICATIONS FOR CROSS BRODER REINSURANCE (CBR)
FOR ACCESSING CBR PORTAL
1. The portal can be best viewed at 1420 x 768 resolution in latest versions of Google Chrome and Firefox Browsers
2. The portal can be accessed at https://cbr.irdai.gov.in/login.aspx.
3. Insurer may use the same User ID/ Password for accessing the portal, which are currently being used by the insurers.
4. Necessary guidance notes for filing the CBR application have been provided below. Insurers are advised to read the instructions stated in the guidance thoroughly, before filing the applications.
5. The portal will be available for access from 23-Jan-2021:09:00 Hrs onwards
In case any technical issues related to accessing of portal, a mail may be sent to ankit@irdai.gov.in under CC to reinsurance@irdai.gov.in
INSURANCE REGULATORY AND
DEVELOPMENT AUTHORITY OF INDIA
Guidance Note
Application filing procedure for allotment of
Filing Reference Number (FRN) to Cross Border
Re-insurers (CBR)
Ver 01
January 2021
The Authority vide Ref. No. IRDA/RI/GDL/MISC/015/01/2021 dated 22-Jan-2021 had notified Guidelines on Cross Border Re-insurer. The insurer who wish to place reinsurance business with CBR shall file an online application with the Authority in the form as specified at Annexure – 1 of the guidelines. To bring consistency in the “data” filed through electronic submission, “Guidance Note on filing the application for allotment of FRN to CBR. While due care had been taken to prepare this Guidance Note, Chief Compliance Officer of the insurer may point out the suitable modifications in this documents which may to be addressed in the subsequent versions.
Screen No. 1 (a)
Objective: On this page it is expected that the complete details of applicant Cross Border Re-insurer (CBR) are to be entered by the insurer who wish to place business with the CBR.

1. All fields in this application form are mandatory;
2. Registration Valid Upto: Certain Home Country Regulators / Supervisors will issue registration to the (Re)insurer for limited period say for one year. While in certain cases such registration may be for indefinite period, in such case insurer may enter this date as 01-Jan-2100;
3. Complete name of Supervisory Authority for the concerned CBR its complete address shall be entered. The name in abbreviated form is not acceptable;
Screen No. 1 (b)
Objective: Same as for Screen No. 1 (a).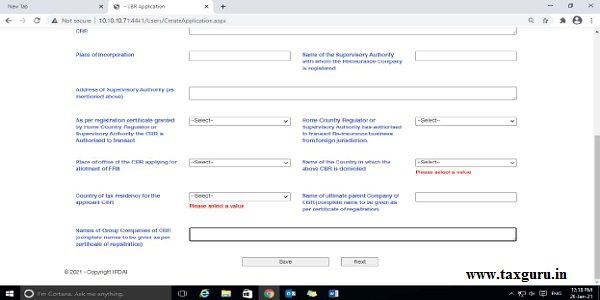
4. Place of Office of the CBR: Place of the specific branch office of CBR applying for allotment of FRN should be entered;
5. Name of Country of Domicile: Country where the CBR’s branch office is domiciled would be required and the same can be enter from the drop-down list.
6. Country of tax residency: This pertains to the country where the branch office of CBR is reporting for tax purpose;
7. Complete name of ultimate parent company is to be entered, name in abbreviated form is not acceptable;
Screen No. 2
Objective: To get valid contact details of the officials who are responsible to handle work portfolio as discussed in the heading.

1. (B) Details of the person responsible for providing requisite information of CBR: Details of the person/ representative of CBR, who is providing all the information about CBR should be entered.
2. (C) Details of the department person responsible for providing confirmation on receipt of premium by CBR: Details of the person/ representative of CBR, who is providing all the information about CBR should be entered.
Screen No. 3 (a)
Objective: To examine financial strength of the CBR.
1. Amount of Paid-Up Capital & Free Reserves as per last audited Balance Sheet: Values in both fields should be entered in home country currency. Ensure not to enter currency name/abbreviation. Only values to be entered.
2. Solvency Ratio: Kindly enter the relevant data in percentage (%) term for last 3 years starting from the year preceding the current year.
Screen No. 3 (b)
Objective: To examine financial strength of the CBR.

1. Incurred Claims Ratio (ICR) & Combined Ratio for last 3 years: Kindly enter the relevant data in percentage (%) term for last 3 years starting from the year preceding the current year.
Screen No. 4
Objective: To examine previous applications filed by the CBR, if any.

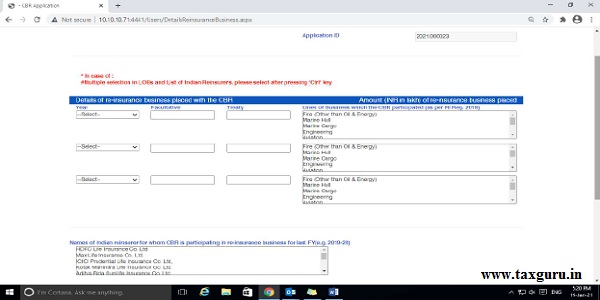
Screen No. 5 (a)
Objective: To ascertain the business relationship of CBR with Indian market.
Screen No. 5 (b)
Objective: To ascertain the business relationship of CBR with Indian market.
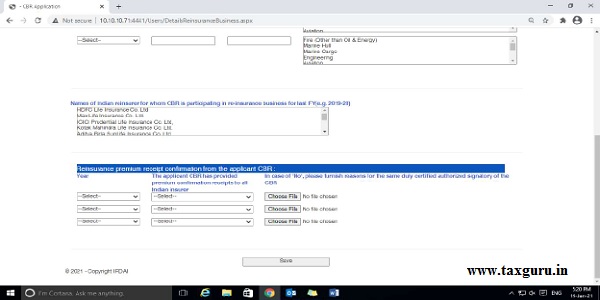
1. Re-insurance premium receipt confirmation from the applicant CBR (B) In case of ‘No’ please furnish reasons for the same duly certified authorized signatory of the CBR:
Kindly upload the required document certified by the “CBR” in each case of “No” (Max File size: 1 MB.)
Screen No. 6
Objective: To examine compliance with eligibility criterial of the CBR:
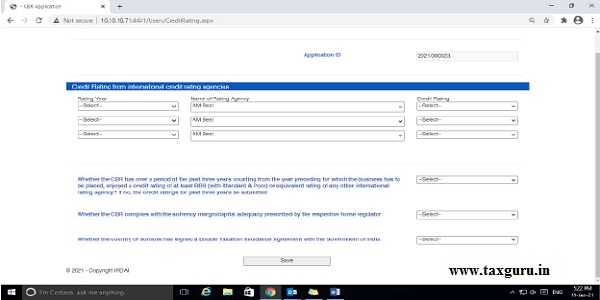
1. Credit rating from international credit rating agencies: Kindly enter the relevant data for last 3 years starting from the year preceding the current year.
2. Ensure accurate data entry in all fields.
Screen No. 7
Objective: Details of Authorized signatory of the CBR.

Screen No. 8 (a)
1. Re-insurance premium receipt confirmation from the applicant CBR
2. (B) In case of ‘No’ please furnish reasons for the same duly certified the Head of Reinsurance Department of the Insurer:
Kindly upload the required document certified by the “Head of Reinsurance Dept. Of applicant Insurer” in each case of “No” (Max file Size : 1 MB.)
Screen No. 8 (b)
Objective: Submissions to be made in case of file application for Non–Eligible CBR.

Screen No. 9

1. The user will be able to view the details of data submitted in the applicable and take printout for records.
2. Once application is submitted, the same will be available for IRDAI user to process the same.
Annexure to IRDAI Guidelines No. IRDA/RI/GDL/MISC/015/01/2021
dated 22-Jan-2021 on CBRs
Annexure – 1
FORM CBR – 1
APPLICATION FOR ALLOTMENT OF UNIQUE REFERENCE NUMBER FOR CBR
This application shall be signed by Authorised Signatory of CBR and Chief Compliance Office of the insurer. Digital Signatures are accepted;
| Application for allotment of FRN for FY | (e.g. 2020-21 and 2021-22) |
| Application for allotment of FRN for Eligible CBR or Non-Eligible CBR | Eligible CBR or Non-Eligible CBR |
–
| Particulars | Details | ||
| A. General Information | |||
| Name of the CBR (as per Certificate of Registration) | |||
| Place of Incorporation | |||
| Date of Incorporation | (dd/mmm/yyyy) | ||
| Address of Registered office of the CBR | |||
| Name and address of Supervisory Authority with whom the Reinsurance Company is registered | |||
| Registration Number & valid upto | _________________valid up to (dd/mmm/yyyy) | ||
| As per registration certificate granted by Home Country Regulator or Supervisory Authority the CBR is Authorised to transact; | Direct Life Insurance; Direct General Insurance; Composite Direct Insurance (i.e. Life & General both) or Re-Insurance Business (Life & General) or Direct and Re-insurance Business both. | ||
| Home Country Regulator or Supervisory Authority has authorised to transact Re-insurance business from foreign jurisdiction. | Yes / No. | ||
| Place of office of the CBR applying for allotment of FRN | |||
| Name of the Country in which the above CBR is domiciled | |||
| Country of tax residency for the applicant CBR | |||
| Name of ultimate parent Company of CBR (complete name to be given as per certificate of registration) | |||
| Names of Group Companies of CBR (complete names to be given as per certificate of registration) | |||
| B. Details of the person responsible for providing requisite information of CBR | |||
| Name | |||
| Designation | |||
| Business phone number | |||
| Address | |||
| Email Id | |||
| C. Details of the department person responsible for providing confirmation on receipt of premium by CBR | |||
| Name | |||
| Designation | |||
| Business phone number | |||
| Address | |||
| Email Id | |||
| D. Financial Position of the CBR | |||
| Details of Capital: | |||
| Amount of Paid-Up Capital: | in INR ___________ | ||
| Free Reserves as per last audited Balance Sheet | in INR ___________ | ||
| Name of Currency in which re-insurance business will be transacted | Conversion to INR _____ | ||
| Solvency Ratio as per home country regulator for last 3 years | Regulatory prescription | Actual Solvency Margin of the CBR | |
| Last year (e.g. year 2019) | |||
| Last to last year (e.g. year 2018) | |||
| Last to last year (e.g. year 2017) | |||
| Incurred Claims Ratio (ICR) for last 3 years | Last Year
(e.g. year 2019) |
Last Year (-) 1 (e.g. year 2018) | Last Year (-) 2 (e.g. year 2017) |
| Details of ICR | |||
| Combined Ratio for last 3 years | Last Year
(e.g. year 2019) |
Last Year (-) 1 (e.g. year 2018) | Last Year (-) 2 (e.g. year 2017) |
| Details of Combined Ratio | |||
| Details of previous CBR FRN as per IRDAI Portal (if any) | Last FY (e.g. FY 2019-20) | Last FY (-) 1 (e.g. FY 2018-19) | Last FY (-) 2
(e.g. FY 2017-18) |
| CBR FRN No. | |||
| Details of previous FRN as per BAP Portal (if any) | Last FY (e.g. FY 2019-20) | Last FY (-) 1 (e.g. FY 2018-19) | Last FY (-) 2
(e.g. FY 2017-18) |
| CBR FRN No. | |||
| Details of re-insurance business placed with the CBR | Amount (INR in Lakh) of re-insurance business placed | ||
| Facultative | Treaty | ||
| Last Year (e.g. 2019-20)
[Year (206-17 onwards) may be given as drop down] |
Lines of business which the CBR participated (as per RI Reg. 2018) | ||
| Last Year (e.g. 2018-19)
[Year (2016-17 onwards) may be given as drop down] |
|||
| Last Year (e.g. 2017-18)
[Year (2016-17 onwards) may be given as drop down] |
|||
| Name(s) of Indian insurer for whom CBR is participating in re-insurance business for last FY (e.g. 2019-20) | Names of Indian insurer | ||
| Re-insurance premium receipt confirmation from the applicant CBR | Last FY (e.g. FY 2019-20) | Last FY (-) 1 (e.g. FY 2018-19) | Last FY (-) 2
(e.g. FY 2017-18) |
| The applicant CBR has provided premium confirmation receipts to all Indian insurer | Yes / No | Yes / No | Yes / No |
| In case of ‘No’ please furnish reasons for the same duly certified authorized signatory of the CBR. | |||
| E. Credit rating from international credit rating agencies | |||
| Name of Rating Agency | |||
| Year of Rating | |||
| Credit Rating | |||
| Whether the CBR has over a period of the past three years counting from the year preceding for which the business has to be placed, enjoyed a credit rating of at least BBB (with Standard & Poor) or equivalent rating of any other international rating agency? If no, the credit ratings for past three years be submitted | (Yes/No) | ||
| Whether the CBR complies with the solvency margin/ capital adequacy prescribed by the respective home regulator | (Yes/No) | ||
| Whether the country of domicile has signed a Double Taxation Avoidance Agreement with the Government of India | (Yes/No) | ||
| DECLARATION CUM UNDERTAKING: I / we solemnly declare that the information supplied in this application form is true and correct. | |||
| Place: | Signature | ||
| Date: | Seal | Name: | |
| Designation: | |||
| [Authorised Signatory of CBR] | |||
| Specific recommendation of the (re)insurer justifying as to why they would like to make Reinsurance placements with the referred CBR even though it does not comply with prescribed eligibility criteria. | |||
| The filing of this application is in compliance with Reg. 5 (2) (B) of the IRDAI (Re-insurance) Regulations, 2018 | (Yes / No) | ||
| In case of No, the insurer has to submit clarification on the matter | Free text | ||
| Re-insurance premium receipt confirmation from the applicant CBR | Last FY (e.g. FY 2019-20) | Last FY (-) 1 (e.g. FY 2018-19) | Last FY (-) 2
(e.g. FY 2017-18) |
| Comments on receipt confirmation from the applicant CBR | Yes / No | Yes / No | Yes / No |
| In case of ‘No’ please furnish reasons for the same duly certified the Head of Reinsurance Department of the Insurer. | |||
| The following are the documentary Requirements in case of Application for Non-Eligible CBR | |||
| Copy of registration Certificate issued to CBR by home country regulatory / Supervisory Authority | |||
| Signed copy of specific recommendation of the insurer, justifying as to why they would like to make Reinsurance placements with the referred CBR. Such recommendation shall necessarily be made by the Head of Reinsurance Department of the Insurer. | |||
| DECLARATION CUM UNDERTAKING BY CMD / CEO OF INDIAN (RE)INSURER:
a. I / We confirm that, before filing the documents with the Authority, we have conducted the required due diligence and have scrutinized the documents pertaining to above CBR. b. We ensure strict compliance with the eligibility criteria for CBRs as prescribed by the Authority in extant regulations / guidelines. (applicable in case if, application filed is for CBR who comply with eligibility criteria); c. I / We undertake that, all information furnished is correct, in the event if it is proved that any information submitted is wrong or incorrect I / we will be liable subject to the provisions of the Act, Regulations and guidelines notified by the Authority. |
|||
| Place: | Signature | ||
| Date: | Seal | Name: | |
| Designation: | CCO | ||
Annexure to IRDAI Guidelines No. IRDA/RI/GDL/MISC/015/01/2021
dated 22-Jan-2021 on CBR
Annexure-2
Certificate of Compliance
Name of Insurer:
Financial Year:
Certified that the company has placed all its reinsurance placements for the Financial year _______ to those CBRs who comply with the;
1. Eligibility criteria prescribed in the extant Guidelines on Cross Border reinsurers; or
2. Who have been specifically approved by the Authority.
All placements made with Cross Border Reinsurers under (2) above, have been approved by the Board of the Company.
Signature
Seal
Name:
Designation: Chief Compliance Office
Place:
Date:


